
A need for better quality, evidence-based, data-led information
The results of the Patient Information Forum (PIF) Maternity Decisions: Induction survey in 2021 were not unexpected but made for sobering reading all the same.
Rates of induction in the UK are rising, but some women ranked fear of induction as one of their biggest concerns as they approached labour and birth. 50% felt they lacked timely information to help them make an informed choice. Less than 20% had any risk/benefit information at all. Many spoke of being ‘told’ they needed an induction or felt coerced into it but were not given enough information about the process. They were not involved in any discussion about the risks and benefits to them and their baby.
This lack of information also meant that those who did have an induction:
- still didn’t feel it was a conscious decision they had made about their care,
- didn’t know what choices they could make throughout the process,
- often felt disempowered and out of control.
The women who completed the survey were very clear about the need to have better quality, evidence-based, data-led information to help them have a supportive conversation. This is an issue which can and must be addressed immediately, so that women can participate equally and make informed choices about their care.
Sue Farrington – Chair, PIF
Norgine UK, who helped fund the survey, also funded Tommy’s to address some of these concerns. I was entrusted with the development of new induction of labour content.
Further research with stakeholders and users
Before I created a content plan, we had some more research to do. I recruited a steering group of wonderful, experienced and knowledgeable women who could provide feedback and suggestions. These included Mars Lord and Leah Lewin who were involved in the Not So Nice campaign (when NICE draft induction guidelines tried to suggest inducing all Black, Brown and Mixed heritage women at 39 weeks in a startlingly blunt attempt to reduce maternal inequalities). Marley Hall and Dr Abi Merriell also kindly gave their time to the initial meeting, along with Dr Alex Freeman and Leila Finkiarides from the Winton Centre for Risk and Evidence Communication in Cambridge.
We were aware the PIF survey was not particularly representative, so we ran our own survey (using the same questions) for women and birthing people of Black, Brown and Mixed heritage. I pulled together a lived experience focus group from these respondents and others from our user review team.
Key additional issues from research
- Importance of risk communication and getting this right, while ensuring the content is still Plain English with a reading age of around 9.
- We need to help people feel confident and comfortable to make a choice and advocate for themselves in situations where they often feel powerless. A decision led by fear is not an informed decision.
- Younger women and birthing people tend to feel even less able to advocate for themselves.
- Amid many other concerns that we are, finally, starting to hear more about, Black and Brown women are more likely to have a negative experience/ be viewed as aggressive and have social services called when they stand up for themselves and ask questions.
- People want more information on timelines – what happens when, how long does it take, what happens if it doesn’t work. Honesty around possible pain levels is important too.
- Medicalised language can and have been used to confuse people and coerce them into uninformed consent if they don’t know what terms mean, or the implications of a procedure.
- Birth partners can play a key role in advocating in the birth room, but only if they are knowledgeable themselves and know what their partner wants and needs.
Induction of labour content development
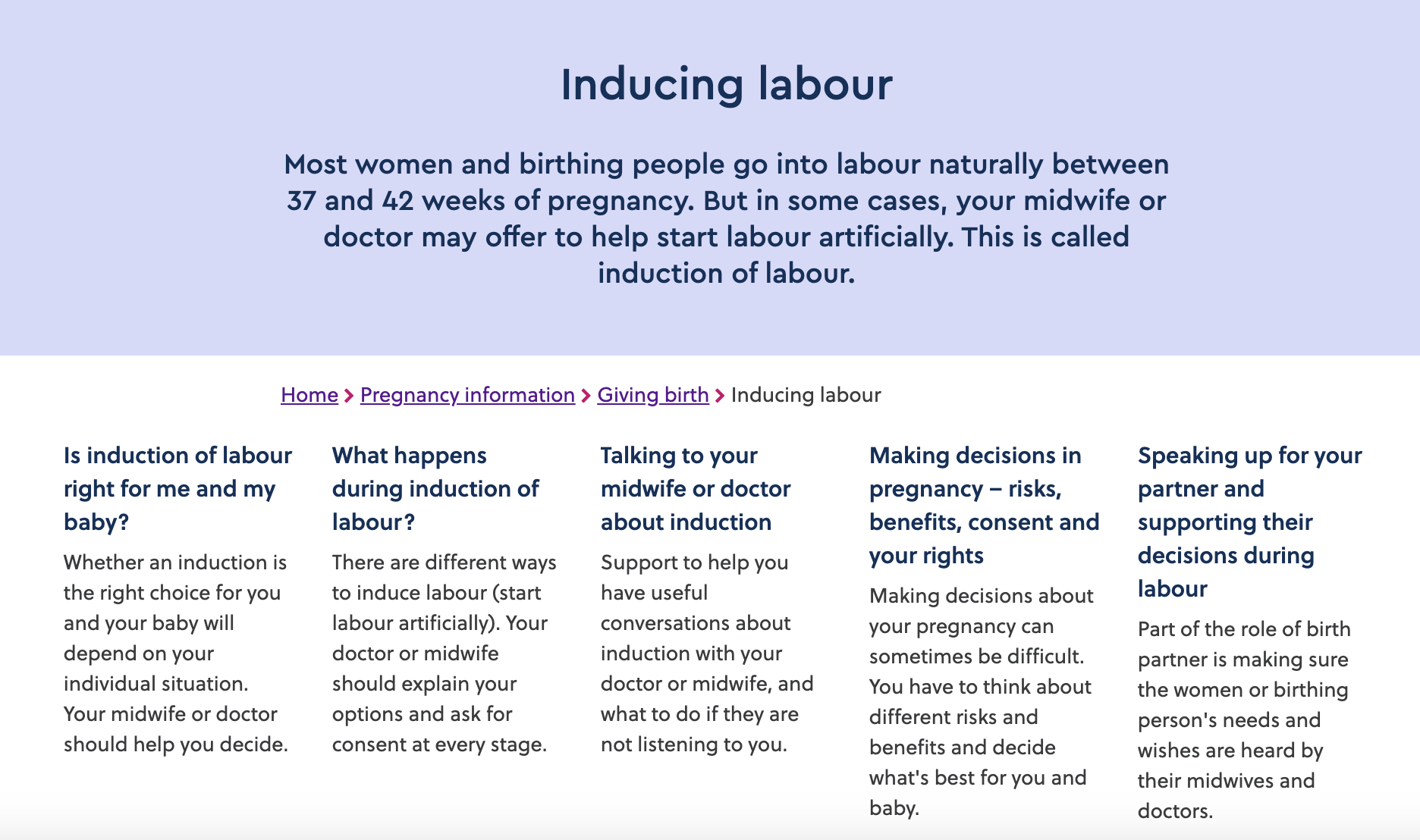
I used our stakeholder and lived experience group discussion, results from the surveys we ran and my own desk research and reading to develop a plan for 5 new content pieces. Tommy’s Information Production Process is accredited by PIF Tick so all content is evidence based and reviewed by the expert steering and user groups, as well as Tommy’s midwives.
Explaining what induction of labour is and different situations where it might be offered and why. Information on the risks and benefits of choosing induction (or not), and any relevant statistics.
What happens when, medical terms, how long could each intervention take and what are the side effects, risks and benefits of each.
Recognising the difficult of these conversations and giving people permission to ask questions and take control of the situation. Providing specific examples of phrases to open or direct the conversation.
Information on what is (and isn’t) informed consent, understanding risk, thinking about your individual situation, taking your time, asking questions and finding out more. I wanted this to be a more general piece that could be useful across Tommy’s pregnancy information. I’m particularly proud of this one.
Another one I hope will be useful across Tommy’s pregnancy information. Support for birth partners in their role as someone who can support the birthing person with decisions and make sure their needs and wishes are heard by those in the room.
Challenges
Controversy around guidelines
Tommy’s information is based in the best available evidence. As are the NICE guidelines – we hope. In almost all cases these converge. But there is enormous controversy among midwives, doctors, researchers and other health professionals around the NICE guidelines for induction of labour. Are they based too much in expert opinion and not evidence? Has the available evidence been interpreted correctly? Are they biased towards intervention?
The content must also recognise the experiences people are having on the ground and meet the needs that arise from that. In this case, the overwhelming majority of people said they had a negative experience, either of induction itself or the conversations that led up to it. Some of these were because the NICE guidelines were being followed, others were because they were not.
We had to recognise the issues these conflicts were based in as well as ensuring people understood the what the NICE guidelines said and why. To do this, I kept the focus very clearly on informed choice, helping people to understand how the guidelines related (or not) to their individual situation, and giving them the tools to think about this for themselves and feel confident to ask useful questions.
I also chose to bring in the voices of those with lived experience alongside the written content. This helped explore the nuances of real experience.
Balance, representation and fear
Some people have a positive experience of induction. All things considered, it is the right choice for them, and they feel informed and included throughout. On the whole, they are probably less likely to respond to surveys and questions about induction than those who have had a difficult experience.
Most healthcare professionals want to do the right thing by their patients. They are not in the business of coercion or disrespect.
We don’t really want to create content that implies otherwise or creates an us vs. them narrative. But we also need to have the courage to recognise the problems and our role in resolving them. To meet the needs so clearly spoken in the surveys and research. To ensure women and birthing people go into these situations informed and prepared, whether it is their first or their fifth time giving birth.
This was a tricky line to tread. But this is also what I love best about developing content. The process of research and reading, the gathering of information and ideas, the challenge of creation and development, discussions and debate, the art of adjusting and amending until we have something that does what we want it to.
I’m not saying I have got it completely right. The feedback, discussion and amendments will continue. But I am proud of where we have got to so far. And the web traffic is looking positive too. Since the new content went online, views have been up 6250.63%, users up 5,446.55% and engagement time up by 155.84%. This suggests we are going some way towards meeting a need and filling that information gap.
